Obsessive Compulsive Disorder
Obsessive Compulsive Disorder (OCD) is a very misunderstood disorder. Unfortunately, there are still a lot of misconceptions about it.
Written by: Anna Zajaczkowska; 11-09-2024
What is OCD?
Obsessive Compulsive Disorder (OCD) consists of two parts - obsessions and compulsions.
Obsessions are repeated intrusive thoughts, mental images and urges. These are ego-dystonic in nature meaning that they go against a person’s values and are unwanted. Everyone gets intrusive thoughts (and the like) from time to time; people with OCD are more likely to become preoccupied with these. Someone with OCD may worry about these thoughts and their meaning, which causes them to develop an obsession. Sometimes these obsessive thoughts come up randomly, but sometimes they may be triggered by some external event or situation (e.g. seeing or talking about something).
Compulsions are actions or rituals that an individual feels compelled to carry out in order to prevent something bad happening or to reduce anxiety. It is important to note that most people with OCD understand that this is irrational and doesn’t make sense. Unfortunately, the urge to carry out a compulsion is very strong and they would still feel that they need to do something ‘just in case’. Resisting a compulsion for someone with OCD is very hard and can result in extreme anxiety or panic.
People without OCD may also experience obsessions and/or compulsions. The disorder part of OCD comes when these obsessions and compulsions start to interfere in daily life. OCD sufferers may have all areas of their life impacted including social, work and personal. Obsessions bring a large amount of distress into their lives and compulsions can take hours and hours worth of time out of their day.
How do I know if I have OCD?
As mentioned above, you must have both obsessions and compulsions that interfere with daily life for you to have OCD. Despite the common stereotype, OCD is not just about cleaning - obsessions and compulsions can concern virtually anything. There are different subtypes of OCD, however the mechanism behind all is the same - it actually does not matter what the content of the obsessions is (and one person can have more than one obsession). What actually matters is the mechanism behind obsessions and compulsions. This is the main way you can identify an obsession or a compulsion.
Subtypes of OCD and possible obsessions:
(TW: mentions uncomfortable topics including suicide, self-harm, harm, sex)
Some common misconceptions about OCD are:
Hidden Compulsions
Some compulsions are more visible, while others are less. This does not make any difference to their nature. The important thing is the role they serve in the mechanism of OCD, which is the same regardless of obsession and compulsion (see below). Some compulsions that are more difficult to notice are listed below:
The mechanism
Disclaimer: Writer is not a medical professional or scientist but the explanation below has been checked by a person with lived experience.
A more scientific decription will be added later
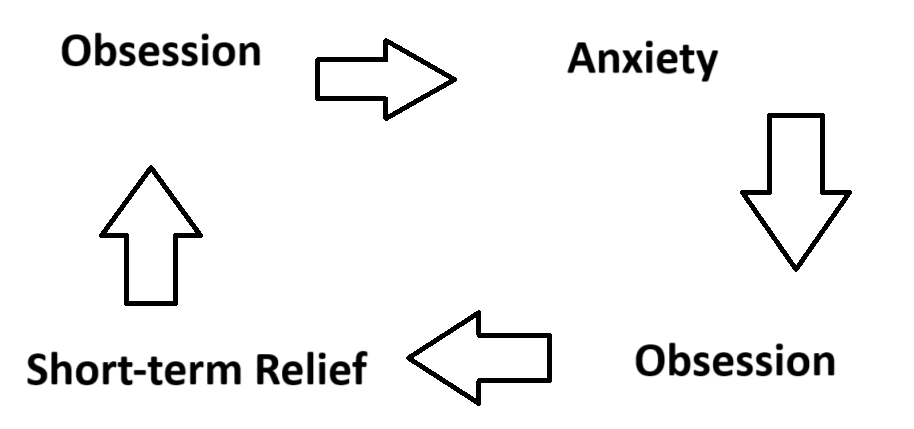
It is important to note that compulsions only give short term relief which is why they are not helpful. Essentially, they drive the OCD cycle. This is because engaging in compulsions reinforces the connection between obsession and compulsion. Compulsions reinforce the thought that the obsessive thoughts are a threat (a misidentification). This makes the cycle stronger and harder to break. Compulsions become stronger and develop - for example more are needed or different ‘stronger’ ones are made. Any external triggers for the obsessions (e.g. seeing something) may also develop and increase in number. The outcome is an increase in severity of the OCD.
Treatment
Disclaimer: Writer is not a medical professional and therefore cannot recommend the following.
The following is simply a collection of common forms of treatment for OCDs
Usually, OCD is treated with therapy - CBT with ERP. ERP is a therapy that deals in Exposure Response Prevention and has so far proved to be the most effective form of therapy for treating OCD. During recovery, an individual with OCD may still have some obsessions and compulsions occasionally but may no longer qualify the criteria for having OCD.
Some people may also find medication (SSRIs) to be helpful. However, it is important to note that this is not a cure and does not make OCD go away. It may reduce the intensity of the obsessions and compulsions.
Comorbidities
OCD is often comorbid with anxiety, depression, ADHD, Autism, BFRBs, BDD and Hoarding disorder.
Support
Please check out our other pages for general support as well.